


ORIGINAL ARTICLES

Introduction. Optic nerve atrophy is a degenerative condition and a prevalent cause of visual impairment, including in children. Data on refractogenesis in schoolchildren with partial atrophy of the optic nerve (PAON) are scarce, with existing literature focusing primarily on the correction of low vision associated with this disorder. Purpose: to assess the refraction dynamics in schoolchildren with congenital PAON over a ten-year observation period.
Materials and methods. We conducted a retrospective analysis of refraction changes over a decade among three groups: 1) 47 schoolchildren with PAON, 2) 49 schoolchildren with ametropia without PAON, and 3) 49 schoolchildren without any ophthalmopathology.
Results. All groups exhibited a trend towards myopization (р < 0.001). In groups with myopic and emmetropic refractions (without ophthalmopathology at the start), either the emergence or an increase in myopic refraction was noted. In hypermetropic children, a gradual decrease towards emmetropic refraction or a shift to myopic refraction was observed. For myopic schoolchildren using contact lenses and perifocal glasses from the ages of 11–13, myopia progression stabilized, particularly with perifocal optical correction (р < 0.01). Despite refractive changes during the school years, regular courses of functional treatment and accommodation training led to a slight improvement in visual acuity in PAON patients (by an average of 0.05 ± 0.01 (p = 0.001) in myopes and 0.06 ± 0.01 (р < 0.001) in hypermetropes) and a significant increase in visual acuity in children with normal fundus ametropia (by an average of 0.14 ± 0.02 (р < 0.001) in myopes and 0.18 ± 0.02 (р < 0.001) in hypermetropes).
Conclusion. The ten-year observation demonstrates a myopization trend in all groups of schoolchildren, which holds particular relevance for those with PAON due to their inherently lower visual acuity. An optimal optical correction strategy, employing modern myopia control measures in tandem with regular functional treatment and accommodation training, is essential for a health-preserving educational approach in schoolchildren with PAON.
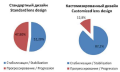
Background. The increasing prevalence of myopia in children highlights the need for effective treatments. Orthokeratology is a key approach to slow myopia progression, yet standard ortho-k lenses often fall short due to diverse corneal structures. Personalized ortho-lens designs are crucial for optimizing myopia control and maximizing the benefits of corneal refractive therapy.
Aim: to evaluate the impact of custom ortho-k lens use on myopia control in children, specifically assessing changes in refraction and axial length during orthokeratology treatment.
Materials and methods. In our study, 41 school-aged children underwent custom orthokeratology treatment with 81 ortho-k lenses. Utilizing a Medmont E300 for corneal topography and the OrthoTool for lens calculations, alongside Lenstar LS 900 for optical biometry, we assessed myopia progression and axial elongation. The subjects’ average age was 12.6 ± 2.4 years, with an average lens wear duration of 17.0 months (range 10.0 to 23.5 months). Initial mean myopia was –5.5 ± 2.0 D in both eyes.
Results. During the study period, 87.8% of the participants (36 children) showed stabilization in refraction and axial length, indicating effective myopia control. However, 12.2% (5 children) experienced myopia progression at a rate of –0.5 diopters per year. Notably, all children undergoing orthokeratology treatment achieved high visual acuity (0.9–1.0). Complications were limited to 12.2% of the participants, who developed mild epitheliopathy (2 degrees) and/or Fleischner rings; no inflammatory complications were observed.
Conclusions. Customized orthokeratology offers significant advantages over standard ortho-k lenses, tailoring treatment to individual corneal structures for more effective myopia control. The results advocate for further, long-term studies into customized orthokeratology and its role in managing myopia.

To date, extensive experience has been accumulated in the correction of high myopia and myopic astigmatism through the implantation of additional negative lenses (phakic intraocular lenses). However, the use of this method in patients with anatomically altered corneas due to keratoconus remains unresolved.
Purpose: to assess the effectiveness and safety of correcting high myopia combined with myopic astigmatism by implanting phakic intraocular lenses in patients with stabilized keratoconus at stages 1–2.
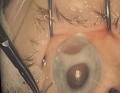
Materials and methods. The study encompassed results from 27 surgeries involving the implantation of phakic intraocular lenses in patients with high myopia and myopic astigmatism (12.63 ± 4.25 D). These patients had thin corneas and were diagnosed with stage 1–2 keratoconus after undergoing corneal collagen crosslinking treatment – this constituted the main group. The control group comprised 35 surgeries performed on patients with subclinical non-progressive keratoconus (Forme Fruste). All participants underwent evaluations for visual acuity dynamics and refractive stability of spherical and cylindrical components before surgery, immediately post-surgery, and then at 1, 6, and 12 months after implantation. Additional assessments included intraocular pressure measurements, gonioscopy, ultrasonic echobiometry, ultrasonic ophthalmoscopy, biomicroscopy, ophthalmoscopy, endothelial microscopy, vision character and stereopsis determination, ultrasound biomicroscopy, anterior segment optical coherence tomography, electrophysiological studies, and statistical analysis. An IPCL (a type of phakic intraocular lenses made from hydrophilic acrylic) was implanted, capable of correcting myopia up to 30 D and astigmatism up to 10 D.
Results. All patients achieved high uncorrected visual acuity 0.86 ± 0.11. Astigmatism correction was successful in 96% of cases. The average postoperative vault – the distance from the back surface of the phakic intraocular lenses to the anterior lens capsule – was 527.5 ± 40.27 μm (range 460–600 μm), and the intraocular pressure was 11.7 ± 2.08 mm Hg. There was a minor decrease in corneal endothelial cell count from 2599 ± 157.3 to 2375 ± 125.3 cells/mm² in the first group and from 2614 ± 104.8 to 2375 ± 43.3 cells/mm² in the second group respectively (p > 0.05), which falls within the acceptable loss range of 4–7% from preoperative values for both groups. Throughout the observation period, there were no cases of cataract development, pigmentary glaucoma, pupillary block, or other vision-threatening complications.
Conclusions. Implantation of phakic intraocular lenses in patients with early-stage stabilized keratoconus and subclinical non-progressive keratoconus provides an effective and practically safe means of correcting high myopia and astigmatism.
Introduction. Iridodialysis refers to a localized detachment occurring at the attachment site of the iris to the ciliary body. This condition is often the most severe consequence of ocular trauma, leading to discomfort, decreased visual quality, and diplopia. Conventional corrective approaches typically induce astigmatism, thereby compromising the functional results of the operation.
Purpose: to assess the effectiveness of an innovative surgical approach for traumatic iridodialysis that incorporates the one-time implantation of a toric intraocular lens in patients with prior unsuccessful cataract surgeries.
Case description. A patient reported significant cosmetic and visual disturbances including reduced visual acuity, photophobia, and visual discomfort in the right eye, following an earlier complicated cataract surgery that did not involve an intraocular lens implant. Our treatment strategy utilized a minimally invasive technique for the simultaneous implantation of the intraocular lens and closed iridoplasty.
Conclusions. The surgical approach provided rapid and complete rehabilitation, yielding high clinical and functional outcomes, including the restoration of visual acuity and the resolution of the patient’s cosmetic concerns.

Introduction. Clinical cases featuring a combination of endocrine ophthalmopathy with a carotid-cavernous fistula are scarce, with only four cases documented in the literature, thus posing a diagnostic challenge due to overlapping clinical symptoms. A carotid-cavernous fistula with high blood flow typically presents a clear clinical picture. However, low-flow variants are challenging to timely diagnose. A history of head trauma can be an essential diagnostic clue, as carotid-cavernous anastomosis develops in 75% of cases post-trauma and in 25% spontaneously. Bilateral carotid-cavernous fistulas are particularly rare.
Purpose: to present the clinical features and outcomes of bilateral endocrine ophthalmopathy associated with a non-traumatic carotid-cavernous fistula, based on the prospective observation of a patient treated in various city healthcare hospitals during 2021–2022.
Case description. The patient first visited the ophthalmologist in October 2021, presenting with bilateral exophthalmos, edema, and eye redness. A positive test for antibodies to thyroid-stimulating hormone and enlargement of the eye muscles, confirmed by orbital ultrasound, led to a diagnosis of “Endocrine Ophthalmopathy”. The patient’s condition was managed jointly by an endocrinologist and an ophthalmologist. Over two months, a worsening of ocular symptoms was observed, prompting a neurosurgical consultation. Cerebral angiography conducted in a hospital setting confirmed a carotid-cavernous fistula. An endovascular procedure was performed five months after the initial ocular symptoms appeared to separate the carotid-cavernous anastomosis on the right using a non-adhesive composition. Ocular symptoms resolved within 2–3 weeks post-surgery.
Conclusions. Clinical manifestations of carotid-cavernous fistulas can resemble those of endocrine ophthalmopathy. The absence of a traumatic head injury history, complaints of unilateral head noise synchronous with the pulse, and the bilateral nature of the symptoms complicated the diagnosis of this neurosurgical pathology in a patient with endocrine ophthalmopathy. It is crucial to include both conditions in the differential diagnosis and to employ a multidisciplinary approach for effective management.
REVIEWS

Since its initial description, Best vitelliform macular dystrophy has been strongly linked to characteristic retinal lesions—subretinal yellowish accumulations, with a hyperreflective structure on optical coherence tomography, situated above the retinal pigment epithelium layer. However, research on this topic remains scarce. It is now recognized that, within the common pathophysiological mechanism of vitelliform lesion formation, this process may contribute to the pathogenesis of a broad spectrum of both genetic and acquired conditions.
The purpose of this review is to update our understanding of genetically determined and acquired retinal diseases associated with the formation of such lesions.
Materials and methods. analysis of scientific publications from databases including PubMed, ScienceDirect, and Cyberleninka was conducted. The review encompasses 16 studies, predominantly from the past decade.
Results. Advances in instrumental and genetic diagnostics have revealed that vitelliform subretinal changes are not exclusive to Best disease but serve as another biomarker, indicating disruption in the metabolism of outer retinal layers. It is hypothesized that, irrespective of etiology, the primary triggering factor for lesion formation is the disjunction of outer segments of photoreceptors and impairment of phagocytic function in retinal pigment epithelial cells. This article presents a contemporary perspective on the presumed etiology and pathophysiology of vitelliform lesions, alongside clinical characteristics, manifestations, and prognosis of diseases associated with this phenomenon. Diseases with identified genetic mutations in the BEST1 gene (Bestrophinopathies) and PRPH2, as well as common acquired conditions like age-related macular degeneration and vitreoretinal traction syndrome, are discussed.
Conclusions. The provided clinical characteristics, supported by multimodal visualization, are expected to aid in differential diagnosis and prognostication of the disease course.
TECHNOLOGIES

We continue to publish works on the properties of materials for gas-permeable contact lenses. In this article, we will explore flexure and the significance of controlling flexure to enable the practitioner to optimise visual outcomes for both corneal and scleral contact lens patients.
LITERARE GUIDE
MEDICINE AND LAW
NEWS: WHAT? WHERE? WHEN?

























