


ORIGINAL ARTICLES
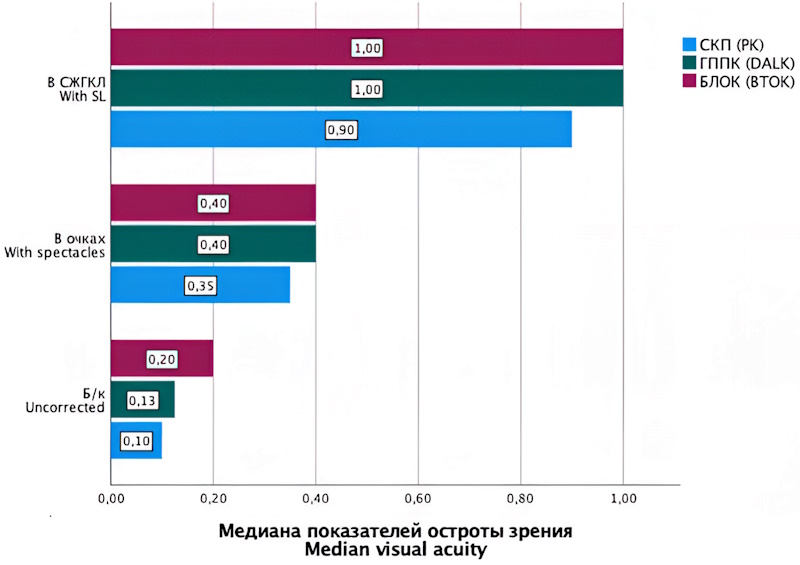
Background. Visual rehabilitation in patients with post-keratoplasty astigmatism remains a major challenge in contemporary ophthalmology. Marked irregularity of the anterior corneal surface after keratoplasty often renders conventional correction methods, including spectacles, soft contact lenses, and corneal rigid gas-permeable lenses, insufficiently effective or unsuitable. Purpose: To perform a comprehensive comparative evaluation of the effectiveness of optical correction of post-keratoplasty astigmatism with scleral rigid gas-permeable contact lenses in patients with a history of keratoconus, according to the keratoplasty technique performed. Materials and methods. This prospective comparative study included 60 patients (60 eyes) with a history of stage III–IV keratoconus who had undergone different keratoplasty procedures between September 2024 and June 2025. The patients were divided into three groups of 20 each according to the keratoplasty technique performed: penetrating keratoplasty, deep anterior lamellar keratoplasty and bandage therapeutic-optical keratoplasty. All patients were fitted with scleral rigid gas-permeable contact lenses. Spherical and cylindrical refractive error, keratometric parameters, visual acuity, and root mean square values for total, lower-order, and higher-order aberrations were assessed before lens fitting and during scleral lens wear. Results. Scleral lens wear resulted in a statistically significant reduction in cylindrical refractive error, keratometric parameters, and total, lower-order, and higher-order corneal aberrations in all three groups (p < 0.001). Visual acuity improved significantly, with a median of 0.9–1.0 across the groups (p < 0.001). Although baseline aberration values were highest in the bandage therapeutic-optical keratoplasty group, final optical correction outcomes were high and comparable with those in the other groups. Conclusion. Scleral rigid gas-permeable contact lenses are a highly effective and versatile option for correcting post-kerato plasty astigmatism in patients with keratoconus. Their efficacy is not influenced by the keratoplasty technique performed.
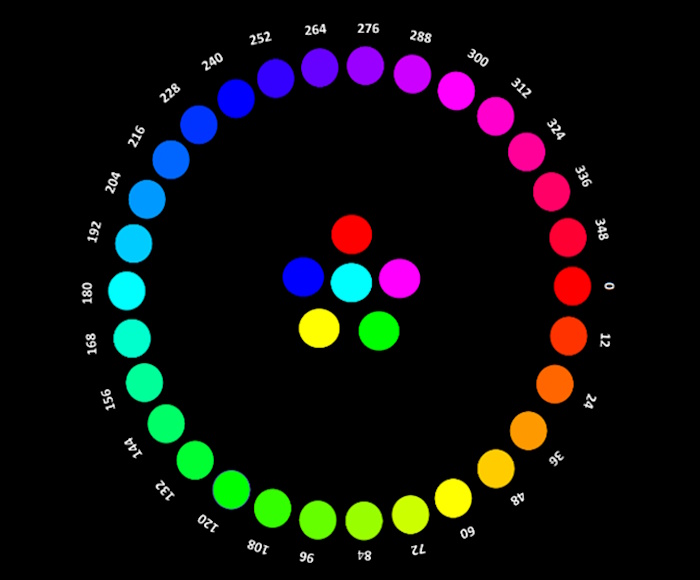
Background. Assessing color vision in children requires a tailored approach: the tests used should be easy to understand, engaging, and quick to administer. The development of effective and practical methods for evaluating color vision in children remains an important objective in contemporary ophthalmology. Purpose: To compare the effectiveness of different methods for assessing color vision in schoolchildren. Materials and methods. A total of 532 schoolchildren (261 boys and 271 girls) with different refractive status were examined. In addition to a standard ophthalmic examination, all children underwent color vision testing using conventional methods (Rabkin pseudoisochromatic plates and the Farnsworth – Munsell Dichotomous D15 test) as well as newly developed tests (a new pseudoisochromatic plate test and a new D30 arrangement test). Results. Among boys, the prevalence of color vision deficiency was 8.1 % with the Rabkin plates, 7.7 % with both the D15 test and the new pseudoisochromatic plate test, and 9.2 % with the new D30 arrangement test. Among girls, the prevalence was 1.1 % according to all tests used in the study. The newly developed tests demonstrated adequate performance in detecting color vision deficiency. For the new pseudoisochromatic plate test, sensitivity ranged from 85.0 % to 88.9 % and specificity from 92.9 % to 99.2 % in children with different refractive status. It also had the shortest administration time across all groups. For the new D30 arrangement test, sensitivity ranged from 80.0 % to 90.9 % and specificity from 96.3 % to 99.6 %. In all groups, its administration time was shorter than that of the conventional tests. Conclusion. The findings demonstrate that the new tests provide high sensitivity and specificity while requiring less time to administer, making them advantageous for large-scale outpatient screening.
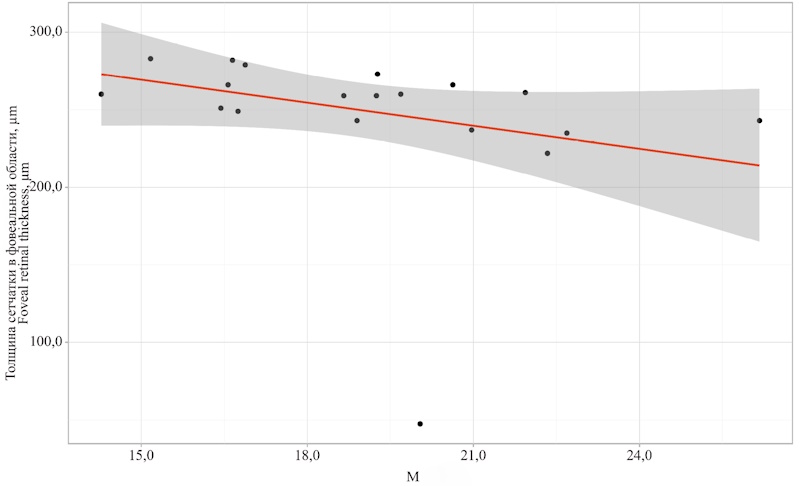
Background. Arterial hypertension is associated with systemic microcirculatory dysfunction, which represents one of the early pathogenetic mechanisms of target organ damage, even in patients who have achieved target blood pressure levels. Ocular microcirculation, which is highly sensitive to systemic hemodynamic and metabolic changes, is regarded as an accessible model for noninvasive assessment of the microvascular bed. Purpose: To assess abnormalities of conjunctival and retinal microcirculation in patients with arterial hypertension. Materials and methods. This single-center observational study, conducted from November 2023 to October 2025, included 22 patients with stage I–III arterial hypertension and 30 healthy volunteers. All participants underwent conjunctival laser Doppler flowmetry (LDF) and optical coherence tomography angiography (OCTA) of the macular region, including analysis of vessel density, perfusion parameters, and the area of the foveal avascular zone (FAZ). Results. Compared with controls (n = 30), patients with arterial hypertension (n = 22) showed reduced conjunctival perfusion (M) (19.88 ± 2.94 vs 21.80 ± 1.17 perfusion units, p = 0.001), reduced blood flow variability (σ) (2.04 ± 0.78 vs 4.91 ± 0.20 perfusion units, p < 0.001), and a lower endothelial component of regulation (5.6 ± 0.56 % vs 9.67 ± 3.34 %, p = 0.001). OCTA revealed a decrease in the superficial retinal capillary plexus vessel density (48.19 ± 1.59 % vs 49.06 ± 0.85 %, p = 0.01) and an increase in interocular asymmetry of this parameter (4.00 ± 4.42 % vs 2.06 ± 1.62 %, p = 0.016) in patients with arterial hypertension. Correlations were found between M and retinal microcirculatory parameters (r ranging from −0.348 to 0.367; p < 0.05). Conclusion. CTA and LDF provide complementary information on structural and functional microcirculatory changes. Their combined use may help detect early vascular remodeling in patients with arterial hypertension and support monitoring of target organ damage.
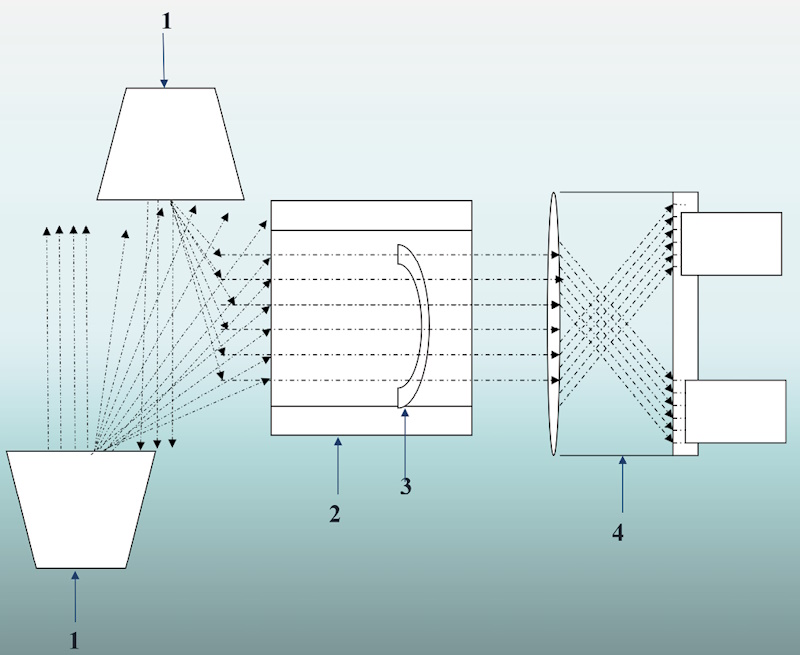
Background. Corneal endothelial dystrophy is one of the most common indications for lamellar keratoplasty. Selection of donor corneal tissue that meets established quality standards is a key step in preoperative preparation. Therefore, the development of new, readily available, and low-cost methods for preoperative evaluation aimed at improving donor tissue assessment remains a relevant and clinically important task. Purpose: To evaluate the effectiveness of retroillumination biomicroscopy in detecting defects in donor corneal tissue compared with conventional slit-lamp biomicroscopy. Materials and methods. Fifty donor corneas were examined using retroillumination biomicroscopy and standard slit-lamp biomicroscopy to identify various corneal defects, including epithelial defects, corneal nerve fibers, corneal scars after radial keratotomy, corneal scars after refractive surgery (LASIK, FemtoLASIK), postoperative scars resulting from tunnel incisions and paracenteses, stromal defects, including opacities, stromal infi ltrates, and endothelial defects, including Descemet membrane folds and localized endothelial damage. Retroillumination biomicroscopy was performed by adding diffuse light sources behind the slit lamp. Results. In donor corneal tissue, retroillumination biomicroscopy allowed significantly more frequent detection of epithelial defects (p = 0.01), stromal changes (p = 0.04), and endothelial defects (p = 0.04) compared with conventional biomicroscopy. Corneal nerve fibers were detected in four cases using retroillumination biomicroscopy and were not identifi ed with slit-lamp biomicroscopy (p = 0.04). Scars after radial keratotomy were detected with the same frequency using both examination methods (p = 1.0). Conclusion. Retroillumination biomicroscopy allows defects in donor corneal tissue to be detected, visualized, and documented with greater accuracy than conventional biomicroscopy. Detection of defects in donor corneal tissue allows preoperative stratifi cation of tissue suitability for different types of keratoplasty.
Background. With the expansion of indications for corneal refractive surgery and the increasing number of procedures performed, the risk of postoperative complications has also increased. One of the clinically significant complications is refractive regression caused by postoperative corneal epithelial hyperplasia. Currently, there are no standardized treatment protocols for this corneal condition. Purpose: To describe a case of refractive regression associated with epithelial hyperplasia after corneal refractive surgery and to evaluate the clinical effectiveness of a proposed conservative treatment regimen. Materials and methods. Using the clinical case presented in this article, we demonstrated the effectiveness of our proposed conservative treatment approach for corneal epithelial hyperplasia in a patient after corneal refractive surgery. The treatment regimen included a course of topical ophthalmic therapy consisting of hyaluronidase (1 vial, 64 IU), dexamethasone eye drops, and 3 % hypertonic sodium chloride solution. Hyaluronidase promotes the degradation of hyaluronic acid, improves tissue permeability, and facilitates normalization of corneal regenerative processes. Results. During treatment, a significant reduction in epithelial thickness was observed on anterior segment optical coherence tomography following completion of therapy. The mean epithelial thickness within the ablation zone decreased from 68 to 56 μm in the right eye and from 71 to 56 μm in the left eye. The patient also reported a marked improvement in visual quality, with no adverse effects observed. The described management strategy demonstrated both efficacy and safety in the treatment of postoperative corneal epithelial hyperplasia after corneal refractive surgery. Conclusion. The proposed conservative treatment approach using hyaluronidase appears to be a promising option for managing postoperative complications after corneal refractive surgery. Further studies and additional clinical observations are needed to refine the indications and optimize the treatment protocol.
REVIEWS
Background. Orthokeratology is one of the most rapidly developing approaches to refractive error correction and myopia control worldwide. Different terminological traditions have emerged, often varying considerably between national ophthalmological schools. As orthokeratology continues to develop, this terminological heterogeneity has become a significant issue. It complicates the comparison of research findings, the conduct of meta-analyses, and the translation of evidence into routine clinical practice. Purpose: To systematize the terminology used in orthokeratology, clarify semantic differences between Russian-language and international concepts, identify controversial definitions, and propose recommendations for the appropriate use of terms in clinical practice and scientific communication. Materials and methods. A targeted search of PubMed/MEDLINE and eLIBRARY.RU was conducted for publications from 1962 to 2025 using the following search terms: orthokeratology, ortho-k, corneal reshaping, reverse geometry, myopia control, ортокератология, and ОК-терапия. The analysis included consensus documents, including BCLA CLEAR Orthokeratology 2021 and the IMI Clinical Management Guidelines 2019, randomized clinical trials, systematic reviews, Russian clinical guidelines, and regulatory documents. Thirty-four peer-reviewed sources that met the inclusion criteria were selected. Results. At least six English-language terms or near-synonyms for the core concept were identified: orthokeratology, ortho-k, corneal refractive therapy, vision shaping treatment, accelerated orthokeratology, and overnight vision correction. Four Russian-language equivalents were also identified: ортокератология, ОК-терапия, ночные линзы and корнеорефракционная терапия. The term orthokeratologist was found to be absent from professional standards in the United States, the European Union, and the Russian Federation and should therefore be regarded as professional jargon used to refer to ophthalmologists and optometrists who practice orthokeratology. The terms open design and closed design were not found in English-language consensus sources. Instead, lens designs are classified by geometric configuration, such as toric or spherical design, and by manufacturing approach, such as stock or custom-designed lenses. Several concepts were found to be insufficiently structured from a semantic standpoint, including the Jessen factor, compression factor, and myopia control efficacy. Conclusion. Standardization of orthokeratology terminology is necessary for the accurate interpretation of clinical studies, transparent communication with patients, and appropriate delineation of professional competencies. In the Russian Federation, the term ophthalmologist specializing in orthokeratology is recommended for use in official documents instead of orthokeratologist. The terms open design and closed design should be replaced with descriptive characteristics of lens design.
Background. Myopia onset and progression are generally associated with school age; however, axial elongation and myopic progression have also been documented in some individuals older than 18 years. Data on myopia in young adults remain limited. Important unresolved issues include the age at which myopia stabilizes after adolescence, the occurrence of incident myopia in young adulthood, the rate of progression, and the identification of risk factors and effective control strategies. Purpose: To synthesize the current evidence on the onset and progression of myopia in adults aged 18 to 40 years and to identify gaps in understanding of risk factors and the effectiveness of myopia control interventions. Materials and methods. A literature review and analysis of original studies indexed in PubMed, MEDLINE, and eLibrary and published between 1987 and 2025 was performed. Eighty-nine publications met the initial inclusion criteria: original studies and reviews; participant age 18–40 years; and quantitative data on changes in refractive error and/or axial length. Of these, 46 studies were included in the final review. Results. Over the past decade, growing evidence has shown that myopia may continue to progress in adulthood, challenging the widely held view that it stabilizes in late adolescence. Clinically meaningful progression can reach approximately 1.00 D between 20 and 30 years of age. Although several myopia control interventions have demonstrated efficacy in children, there is currently no convincing evidence supporting their use in young adults. Factors potentially associated with myopia progression in this age group include genetic predisposition, demographic characteristics, and environmental exposures. Conclusion. Myopia progression in young adults is clinically relevant, but the timing of stabilization and the underlying risk factors remain poorly understood. Further studies are needed to identify structural and biometric predictors of axial elongation and to evaluate the effectiveness of myopia control strategies in young adults.
Background. Glaucoma is one of the leading causes of blindness and visual impairment worldwide. As of January 1, 2022, approximately 1.2 million people with glaucoma were registered in the Russian Federation, including 101 000 individuals with visual disability. The rising prevalence of glaucoma is associated with population aging and a high burden of comorbidity in older adults. This makes the search for new approaches to preventing glaucoma-related blindness and improving glaucoma treatment particularly relevant. Purpose: To investigate the association between statin use and the development or progression of glaucoma. Materials and methods. A systematic literature search was conducted in PubMed, Google Scholar, Web of Science, Scopus, and eLibrary for publications from 2000 to 2025. The search terms were glaucoma, statins, cholesterol, and primary openangle glaucoma. Eligible publications included original studies, meta-analyses, and systematic reviews examining the association between statin use and glaucoma. Overall, 38 publications were included, of which 25 were original studies. Results. Most of the studies reviewed suggest a potential protective effect of statins in glaucoma. Long-term statin use, defi ned as treatment for more than 2–3 years, was associated with a 21–40 % lower risk of developing primary open-angle glaucoma. Several mechanisms have been proposed, including neuroprotection of retinal ganglion cells through improved microcirculation and reduced apoptosis and cytotoxicity; modulation of immune responses; and a potential reduction in intraocular pressure through improved aqueous humor outfl ow. Conclusion. This literature review indicates a complex and heterogeneous association between statin use and open-angle glaucoma development. Although most findings suggest a potential benefit, the evidence remains inconsistent. Large randomized clinical trials are needed to confirm the neuroprotective effects of statins in glaucoma. The available data may inform the development of new statin-based therapeutic strategies for glaucoma management.
TECHNOLOGIES

The article discusses the importance of high oxygen permeability (Dk) for modern rigid contact lenses, especially in conditions of night wear (orthokeratology) and the use of scleral lenses. The use of silicone monomers such as Styrl TRIS makes it possible to achieve Dk values up to 180–250 while simultaneously improving lens stiffness and wettability. New developments from Contamac (Optimum Infi nite and Optimum Breathe) provide safe corneal oxygenation even with increased lens thickness.
WORKSHOP
The article presents a clinical and practical review of the problem of non-compliance with recommendations in contact lens vision correction. The main forms of non-compliant patient behavior, their prevalence, and clinical consequences are discussed. Factors influencing the level of compliance are analyzed, with an emphasis on behavioral and organizational aspects of everyday clinical practice. Special attention is paid to practical strategies for improving adherence to recommendations, including optimization of clinician-patient counseling, patient education, and the rational selection of contact lens correction methods that reduce the dependence of safety on user behavior.
MEDICINE AND LAW
NEWS: WHAT? WHERE? WHEN?

























